A Neuromuscular Therapy Approach to Scapular Dyskinesis
Joints of the Shoulder
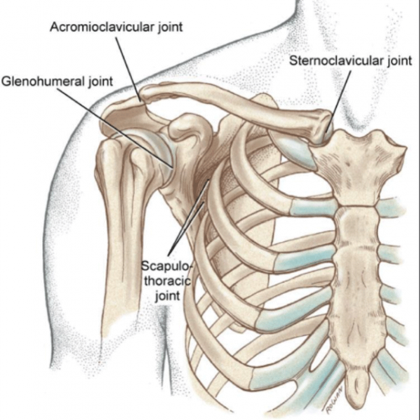
The glenohumeral joint is the most mobile in the body. Its ability to function efficiently is dependent on the scapulothoracic articulation. These are two joints found within the shoulder girdle/pectoral girdle. The other two joints include the sternoclavicular joint and the acromioclavicular joint. The glenohumeral joint has sacrificed stability for mobility which makes sense because the joint is not primarily a weight-bearing joint. Losing function in the shoulder can be a heavy emotional burden.
As adults, our independence is valuable and to lose the ability to reach for and manipulate objects due to shoulder pain can create a great deal of stress and anxiety. It is possible, many of our clients will develop compensatory habits to make up for the lost ranges of motion and may be unaware of actual glenohumeral joint deficiency. For example, if a client needs to reach something in a cupboard and they’ve lost some abduction or flexion, it is likely they will begin laterally flexing or extending the spine in order to complete the motion.
This can happen so gradually that the client is completely unaware of this compensatory behavior. It could occur with such frequency that they develop back pain and schedule appointments to manage that discomfort when it is actually due to a lack of mobility in the shoulder.
Anatomy Review
Let’s begin this dive into scapular dyskinesis by first reviewing the structure of the shoulder girdle. We spoke earlier about the joints involved, so let’s take one step back and consider the bones. There’s the sternum, clavicle, humerus, and scapula. These bones comprise the 4 articulations within the shoulder girdle. Now, we’ll take a close look at the joints they create and the movements at each joint.
Sternoclavicular Joint
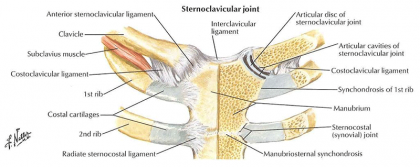
The Sternoclavicular (SC) joint is the synovial joint located at the articulation of the sternum and clavicle. This joint’s claim to fame is that it is the only true articulation that connects the upper limb to the axial skeleton. This is a gliding joint with an articular disc and it is capable of anterior and posterior rotation, elevation and depression, and protraction and retraction. These movements are very closely related to the movements of the scapula. While there aren’t any muscles that directly create movement on the SC joint, several muscles attach to the clavicle which means they may produce movement of the clavicle. Those muscles include:
- Trapezius
- Pectoralis Major
- Scalene
- Sternocleidomastoid
- Deltoid
- Subclavius
Acromioclavicular Joint
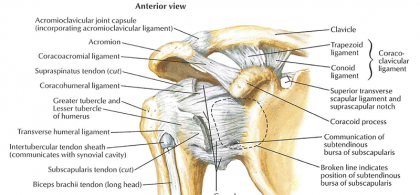
The next joint to review is the Acromioclavicular (AC) joint. This joint is created by the articulations of the clavicle with the acromion process. This gliding joint is primarily responsible for giving the scapula additional rotation on the thorax, disbursing forces from the upper extremity into the clavicle, and creating adjustments in the scapular motion against the ribs. As we consider the movement of this joint, it is important to understand it is going to act in conjunction with the SC joint as well as the scapulothoracic articulation.
Therefore, it’s movements are going to be closely related to those of the SC joint; upward and downward rotation, internal and external rotation, anterior and posterior tilting of the scapula. The muscles involved with movement at the AC joint include the muscles attached to the clavicle and two of those muscles also attach to the acromion process; those are the upper trapezius and the deltoid.
Glenohumeral Joint & Scapulothoracic “Joint”
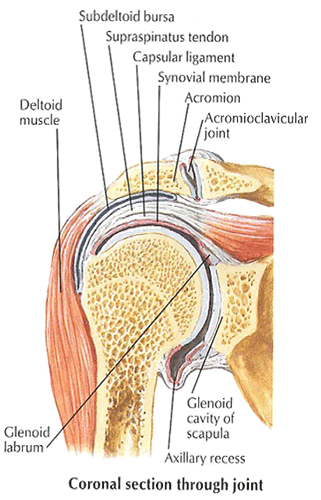
That takes care of the two smaller articulations, now let’s review the two main joints in this area, the glenohumeral (GH) joint and the scapulothoracic (ST) “joint.” Yes, the word joint is in quotation marks; more on that in a little bit. The GH joint is the articulation of the humerus with the glenoid fossa. The glenoid fossa is a relatively flat surface surrounded by the glenoid labrum which serves to “deepen” the joint to allow for better articulation with the humerus. The numerus ranges of motion available at this most mobile joint in the body are:
- Flexion and Extension
- Abduction and Adduction
- Medial Rotation and Lateral Rotation
- Horizontal Adduction and Horizontal Abduction
When we consider the musculature of the GH joint, they should be broken down into two different categories; those that stabilize the joint and those that move the joint. This next part may surprise you. The muscles that are responsible for joint stability and maintaining the position of the humerus in relation to the scapula are the rotator cuff muscles:
- Supraspinatus
- Infraspinatus
- Teres Minor
- Subscapularis
These muscles, contrary to the perception of their group name, are actually more vitally involved in joint congruency than joint movement. The muscles that are primarily responsible for movement in the GH joint are:
- Deltoid
- Pectoralis Major
- Latissimus Dorsi
- Teres Major
- Coracobrachialis
- Biceps Brachii
- Triceps Brachii
Now a quick review of the final joint of the shoulder girdle, the scapulothoracic (ST) “joint.” Remember, this is more of an articulation than a joint because there is no joint capsule. In fact, when we consider that no true bony articulation exists between the scapula and the ribs, there is a lot of mobility here as well. The scapula is capable of:
- Upward Rotation and Downward Rotation
- Abduction (Protraction) and Adduction (Retraction)
- Elevation and Depression
- Anterior Tilt and Posterior Tilt
The important frame of reference when discussing the position of the scapula is the position of the glenoid fossa. While the lack of bony articulation allows for this free movement, it also creates a greater susceptibility to injury because the position of the scapula is floating and not fixed. The rotator cuff muscles, which again, are responsible for GH congruency contribute to scapular position; however, the main muscles required for scapular stability are the:
- Serratus Anterior
- Rhomboid Major and Minor
- Levator Scapula
- Trapezius
Serratus Anterior and Subscapularis
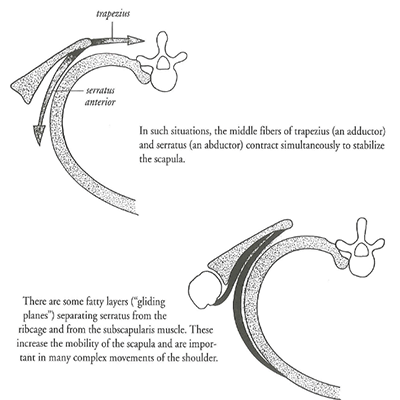
Stability via the Serratus Anterior & Subscapularis
There is a very interesting mechanism of stability that is provided by the serratus anterior and the subscapularis. They provide a suction effect on the scapula which in turn holds it close to the thorax and supports the gliding motion of the scapula over the ribs.
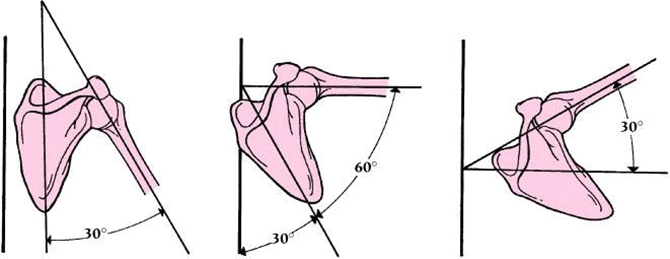
As we have reviewed the anatomy of the pectoral girdle, there’s one relationship we have yet to examine; the correlation between the movement of the humerus and scapula. This scapulohumeral rhythm is the interaction between the scapula and the humerus during movement. During the initial 30° of glenohumeral abduction, the scapula does not move. From 30° to 90° of GH abduction, the scapula will move 1° for every 2° of humeral movement. During movement beyond 90° of abduction, 1° of humeral movement is equal to 1° of scapular movement.
Altered biomechanics, or Pathomechanics, that are attributed to overuse injuries involved in the shoulder girdle have been traced back to alterations in the function of the muscles that stabilize the scapula. The term Scapular Dyskinesis is associated with altered scapular motion and position.
There are multiple contributing factors to the development of Scapular Dyskinesis; these can include bony concerns, which include posture and fractures as well as joint related kinematics which can include AC or GH instabilities, arthrosis, and joint internal derangement. Neuropathy affecting the muscles that stabilize the GH and ST are of major concern as well.
Altered Scapular Motion and Position
Scapular Dyskinesis Etiology
When discussing the etiology of scapular dyskinesis, the acronym S.I.C.K. scapula is used. The acronym indicates the symptoms and signs one might observe during a shoulder evaluation.
- Scapular malposition
- Inferior medial scapular winging
- Coracoid tenderness
- Kinesis abnormalities of the scapula
These changes typically occur in response to repetitive use, especially in athletes that regularly use overhead movements. These strains on the articulation are detrimental to the overall normal function and increase the risk of injury. When considering the S.I.C.K. acronym, signs and symptoms such as a slouched postured, prominent inferior scapular boarder, posterior tipping of the scapula, and scapular winging may be observed.
Further Considerations
A Neuromuscular Therapist would be concerned with a serratus anterior that may be overly lengthened or dysfunctional which would cause the scapular winging. It would also be useful to note if there was any pain during abduction and external rotation. Simultaneously, the winging of the scapula may become more pronounced with muscular fatigue which may contribute to impingement and rotator cuff injury.
It will be important to address the muscles listed above that provide support to the scapula; once the scapula is anchored properly; appropriate kinematics can be restored to the GH joint which will then provide effective and efficient shoulder mobility.
To learn more about Neuromuscular Therapy and the Shoulder, contact the National Holistic Institute Admission Department. The Advanced Neuromuscular Therapy Program in Sacramento is starting the Shoulder/Thoracic Module in December.
Get the details about NHI’s Advanced Neuromuscular Therapy Program and its value in restoring function and addressing chronic pain today. Complete this form to connect with an admissions representative.