“Massage Therapist Thumb” from a Neuromuscular Therapy Perspective
Our hands are our most important tools. We tend to forget how much they do until we have an injury; then even the most mundane task of buttoning a shirt, opening a jar, pouring coffee, or turning a doorknob can become difficult. As Massage Therapists we have to be very aware of how often we use our thumbs in our work; one of the primary reasons Therapists leave the industry is injury. We’re going to look at De Quervain’s Tenosynovitis, or “Massage Therapist Thumb” and discuss methods that can be used to avoid this overuse injury in our profession.
What is De Quervain’s Tenosynovitis?
The exact cause of De Quervain’s Tenosynovitis isn’t known, repetitive wrist and hand movements typically exacerbate the symptoms.
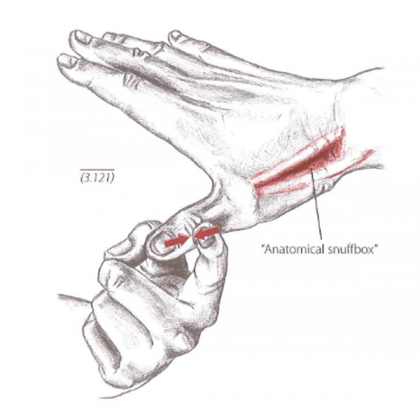
Essentially, De Quervain’s Tenosynovitis is the swelling of the tendons that run along the radial side of the wrist and attach to the base of the thumb; this includes the synovial sheath that covers the long tendons of the Abductor Pollicis Longus and the Extensor Pollicis Longus.
These structures create the “anatomical snuff box.” This structure can be found by abducting and extending the thumb while observing the dorsal aspect of the hand.
How do I Know if I Might Have De Quervain’s Tenosynovitis?
The symptoms will typically cause pain and tenderness along the radial side of the wrist and are particularly aggravated by:
- Moving the thumb
- Forming a fist
- Grasping and gripping
- Turning of the wrist
- Lifting something with your arms in front of you and thumbs pointed towards the ceiling
Ways Massage Therapists Should NOT Use Their Hands
Considering how much work Massage Therapists tend to do with their thumbs in an unsupported position, it is no surprise that this condition is one that would be common within the profession. Here are a few images that demonstrate an unsupported thumb position:
 The downward force on either the finger or the thumb will for the thumb to abduct and extend; not only is the thumb not supported, the line of force would cause the shoulder to medially rotate and cause a lot of muscle recruitment and potential elbow and shoulder injury.
The downward force on either the finger or the thumb will for the thumb to abduct and extend; not only is the thumb not supported, the line of force would cause the shoulder to medially rotate and cause a lot of muscle recruitment and potential elbow and shoulder injury.
 With both of these hand positions, the line of force is definitely more appropriate than the image above; however, the right hand will experience a great deal of tension while the thumb is being abducted and pushed directly into the upper trapezius.
With both of these hand positions, the line of force is definitely more appropriate than the image above; however, the right hand will experience a great deal of tension while the thumb is being abducted and pushed directly into the upper trapezius.
 While some will argue that the stacked thumbs provide support; observe the flexion of the left thumb and the hyper-extension of the right thumb. Additionally, both thumbs are abducted from the hand. This false sense of security may cause Therapists to believe they’re able to apply greater force which can lead to additional injury.
While some will argue that the stacked thumbs provide support; observe the flexion of the left thumb and the hyper-extension of the right thumb. Additionally, both thumbs are abducted from the hand. This false sense of security may cause Therapists to believe they’re able to apply greater force which can lead to additional injury.
 This image is causing all the chills. Not only are we concerned about the development of “Massage Therapist Thumbs” with the hyper-extension of the thumbs; the positioning of the hands and hyper-extension of the metacarpophalangeal joint look excruciating.
This image is causing all the chills. Not only are we concerned about the development of “Massage Therapist Thumbs” with the hyper-extension of the thumbs; the positioning of the hands and hyper-extension of the metacarpophalangeal joint look excruciating.
Proper Use of Hands During Massage Therapy
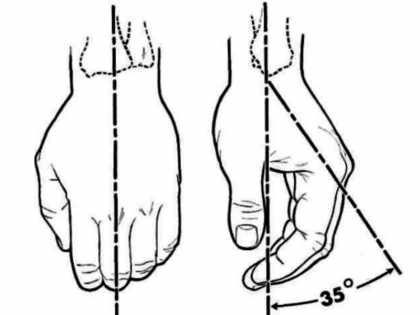 Now, if we’ve identified how hands should not be positioned while practicing Massage Therapy, then what is appropriate? First, let’s take a look at the neutral position of the hand and wrist. Medical texts refer to the functional position of the hand where the wrist is extended 20°-35° and a normal transverse arch is maintained while the thumb is abducted and aligned with
Now, if we’ve identified how hands should not be positioned while practicing Massage Therapy, then what is appropriate? First, let’s take a look at the neutral position of the hand and wrist. Medical texts refer to the functional position of the hand where the wrist is extended 20°-35° and a normal transverse arch is maintained while the thumb is abducted and aligned with  the pads of the four fingers. The proximal interphalangeal joints are flexed to 45°-60°.
the pads of the four fingers. The proximal interphalangeal joints are flexed to 45°-60°.
Essentially, when the hand is placed on a flat surface palm down, we should see slight wrist extension, the pads of the four fingers touch the surface while the thumb rests on its lateral surface while the pad of the thumb points inward. Anatomically speaking, the wrist is an extension of the radius; all force that is generated in the hand travels up the radius to be disbursed into the elbow and shoulder.
 Numerous hand positions can be used while performing Neuromuscular Therapy. Even though it appears the thumb is being used on the left hand in this image; the hand and thumb are still in their neutral positions. The right hand is utilizing a technique called “second thumb” where the index and ring finger tips are held side by side and the middle finger is arched over.
Numerous hand positions can be used while performing Neuromuscular Therapy. Even though it appears the thumb is being used on the left hand in this image; the hand and thumb are still in their neutral positions. The right hand is utilizing a technique called “second thumb” where the index and ring finger tips are held side by side and the middle finger is arched over.
This provides a broader touch surface to address areas that may be hyper-sensitive and it also serves as an excellent tool to “pin” ropey tissue. The combination of hand positions over the sensitive skin on the dorsum of the foot provides a diffused sense of pressure over the tendinous structures over the tarsals.
 In this image to the left, one can misinterpret the thumb acting alone on the plantar aspect of the foot. Take notice that the hand and thumb are still in their natural resting position.
In this image to the left, one can misinterpret the thumb acting alone on the plantar aspect of the foot. Take notice that the hand and thumb are still in their natural resting position.
The wrist is slightly extended and the force going into the foot has an unobstructed flow down the shoulder, through the elbow, to the wrist, and out the thumb. Any movement generated from the feet and hip create micro-movements at the thumb and eliminate the need to flex and extend the interphalangeal joint of the thumb.
 Here we have an example of the use of finger tips side-by-side. Both hands and wrists are in a neutral and relaxed position while deep transverse friction is applied to the medial longitudinal arch and to the attachment of the Tibialis Anterior.
Here we have an example of the use of finger tips side-by-side. Both hands and wrists are in a neutral and relaxed position while deep transverse friction is applied to the medial longitudinal arch and to the attachment of the Tibialis Anterior.
The efficacy of this hand position to introduce touch, palpate, and apply acceptable force to the tissue make it a valuable tool while applying Neuromuscular Therapy. With many Therapists struggling with limited intake and evaluation time, combining palpation into a massage stroke can reduce tissue warming and softening time.
These activations and perpetuating factors must be considered while determining appropriate intervention for De Quervain’s Tenosynovitis. It is imperative that Massage Therapist maintain neutral thumb and wrist positions while applying any modality. When Therapists leave the thumb unsupported, the muscles that become overused which are directly related to De Quervain’s Tenosynovitis are the Abductor Pollicis Longus and the Extensor Pollicis Longus.
Which Muscles are Involved?
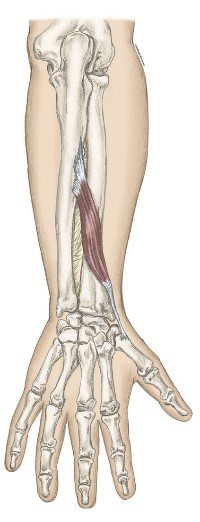
 The Abductor Pollicis Longus is found on the radius, ulna, and interosseous membrane and travels to the base of the first metacarpal. As its name indicates, it is the abductor of the thumb. This muscle is deep to the superficial finger extensors on the posterior aspect of the wrist.
The Abductor Pollicis Longus is found on the radius, ulna, and interosseous membrane and travels to the base of the first metacarpal. As its name indicates, it is the abductor of the thumb. This muscle is deep to the superficial finger extensors on the posterior aspect of the wrist.
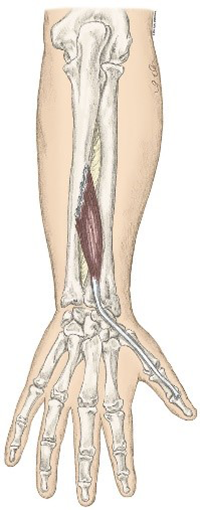
The Extensor Pollicis Longus is located on the posterior ulna and interosseous membrane and goes beyond the Abductor Pollicis Longus attachment to the base of the distal phalanx of the thumb. Just like Abductor Pollicis Longus, the name tells us exactly what the muscle does; it will extend the thumb at the interphalangeal joint and extend the thumb at the metacarpophalangeal joint.
Check out our Instagram and Facebook to see videos of Manual Therapy techniques to address these muscles and De Quervain’s Tenosynovitis.
Ready for more? Get all the details about NHI’s Advanced Neuromuscular Therapy Program now. Complete this form to connect with an Admissions Representative.